

Coronavirus Disease (COVID-19) is a virus that was first identified on January 13, 2020 as a result of research conducted in a group of patients who developed respiratory symptoms (fever, cough, shortness of breath) in Wuhan City (Chine) in late December. Intensive care units have been an important step in combating the COVID-19 pandemic, which rapidly spread worldwide. Although the intensive care requirement of COVID-19 cases varies in different countries, it is stated that hospitalization and intensive care requirements are quite high. It is stated that 54% of COVID-19 patients in Italy had to be hospitalized and 18% of them needed intensive care. COVID-19, an infectious disease that caused more than ten million cases and more than 500,000 deaths worldwide, continues to spread as a global pandemic.
- INTENSIVE CARE UNIT ADMISSIONS OF PATIENTS WITH COVID-19
According to the report published by the World Health Organization; 5% of COVID-19 patients in China and 7-12% in Italy and Spain were admitted to the Intensive Care Unit (ICU) for emergency tracheal intubation due to sudden and severe hypoxia.
In our country, there are no precise data regarding ICU hospitalization and mortality rates regarding COVID-19 patients. The guidelines regularly updated by the Turkish Ministry of Health determined “Patients who should be Evaluated in Terms of Intensive Care Needs” (Table-1). According to the guideline; it’s recommended for patients which suits to determined criteria to be consulted by an intensive care physician. The admission to the intensive care unit should be made if needed according to the intensive care physician sight.
Table 1- Patients who should be Evaluated in Terms of Intensive Care Needs
- Patients with dyspnea and respiratory distress
- Respiratory rate ≥ 30 / min
- PaO2 / FiO2 <300
- Increasing oxygen need
- Despite 5 L / min oxygen therapy patients with SpO2 <90% or PaO2 <70 mmHg, Hypotension (systolic blood pressure (SBP) <90 mmHg and more than 40 mmHg drop from usual SBP and mean arterial pressure <65 mmHg, tachycardia> 100 / min.
- Patients with acute organ dysfunction such as acute kidney injury, acute liver function test disorders, confusion, acute bleeding diathesis and immunosuppression
- Troponin elevation and arrhythmia
- Lactate > 2 mmol
- Presence of skin disorders such as cutis marmaratus and capillary refill disorder
COVID-19 agent (SARS-CoV-2) is a zoonotic virus. It is transmitted from person to person via droplets, direct contact and in some cases via aeosols. Therefore, standard droplet and contact isolation precautions should be taken in cases where COVID-19 is suspected.
Since the virus withdrawal and transmission period is not known, isolation measures should be pursued during all patients’ stay in the healthcare institution (from admission to discharge).
ICU preparation should be completed prior to admission of the patients and in the meantime healthcare workers safety should be a priority. Nurses, physicians and other healthcare workers in the ICU should ensure their safety during all treatment and care giving process by all necessary personal protective equipment (PPE).
- NURSING CARE OF ICU PATIENT DIAGNOSED WITH COVID-19
2.1 Infection Control
According to given data the viral load of severe COVID-19 patients followed in the intensive care unit is 60% higher than the moderate patients, so the viral load is a determinant in the severity and prognosis of the disease. According to the researches patients with a high viral load, especially in the upper respiratory tract, show a higher risk of virus transmission. Patients with suspected or confirmed COVID-19 in ICUs should ideally be treated in a negative pressure room to reduce exposure to aerosols and droplets. Conditions and attempts that cause aerosol generation increase the risk of contamination. Applications that cause aerosol generation are as follows (Table-2);
Table 2- Applications that Causes Aerosol Generation
Endotracheal intubation Nebulizer therapy
Manual ventilation prior intubation Bronchoscopy
Open endotracheal suction Prone positioning the patient
Non-invasive positive pressure ventilation Cardiopulmonary resuscitation
Tracheostomy
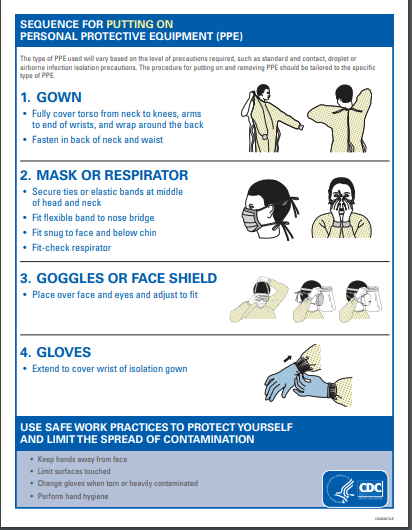
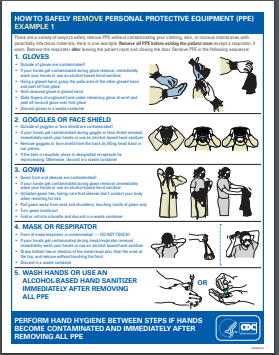
Due to the proximity of the patient’s facial area during these procedures, intensive care professionals should definitely don and doff Personal Protective Equipment (PPE) in the appropriate order. It is very important to comply with hand hygiene during don and doff of PPE.
Personal protective equipment (non-sterile long gloves, non-sterile and preferably liquid-proof long-sleeved gown, medical mask, N95 / FFP2 or N99 / FFP3 mask, face shield, goggles, alcohol-based hand sanitizer) should be kept ready at the entrance of each patient room.
People quantity and entrances to the room should be limited. Physicians and nurses should cooperate to reduce room circulation. Treatment, intervention and other caregiving applications should be scheduled for certain hours and room stay length should be arranged. The door should be kept closed during and after all operations. After aerosol generating procedures the room should be adequately ventilated with natural air flow. After admission cards with warning and precaution information should be placed at the door. Medical materials and medicines should be available in the patient room and should not be taken out of the room.
Preparation and morgue transfer procedures of all patients with suspected or confirmed COVID-19 death should be performed in accordance with the contamination risk procedures. Cleaning and disinfection of all medical equipment and patient unit should be provided daily and when the patient is transferred, discharged or dead. Patient should be restricted to stay at his/her room unless necessary exit for medical reasons. When the patient needs to leave the room (MR, radiological examination, etc.), him/her should wear a mask and contact and droplet isolation precautions should be followed. Visitors are not allowed to the intensive care unit. However, in very special cases (for example farewell), the necessary protective equipment should be put on and allowed. Two separate medical waste bins should be available at the entrance and in the patient room for disposal of the PPEs used. Stethoscope, thermometer and other medical materials should be used exclusively for the patient and should not be taken out of the room. If it’s for common usage it must be cleaned and disinfected after each use (e.g. with 70% ethyl alcohol).
2.2 Ventilation Support
Symptoms of COVID-19 infection can be mild, moderate and severe. Severe illness may be presented with severe respiratory tract infection (severe pneumonia), Acute Respiratory Distress Syndrome (ARDS), sepsis, septic shock, myocarditis, arrhythmia and cardiogenic shock, metabolic acidosis and coagulation dysfunction or other multiple organ failures. Respiratory failure is often seen as hypoxemic respiratory failure and less commonly in the form of hypercapnic respiratory failure. In addition, decompensated heart failure, myocarditis, arrhythmia, acute kidney injury and chronic lung disease exacerbation may be seen in those patients.
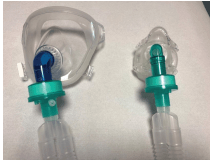 In patients not experiencing dyspnea, hypoxemia can be treated by increasing the FiO2 ratio. In these patients, O2 can be achieved at a rate of> 85% with a flow rate of 10-15 L / min by using a non-rebreather reservoir mask (bag). But during the use of a mask with reservoir, giving O2 over 60% for more than 6 hours may cause oxygen toxicity. In patients experiencing dyspnea noninvasive respiratory support systems are usually used. In conscious patients; in addition to the reservoir oxygen mask a high flow nasal cannula (High Flow Nasal Cannula-HFNC) that can supply 21-100% O2 with a flow rate of up to 60L / min, continuous positive airway pressure (CPAP) or non-invasive mechanical ventilation (NIMV) is implemented. Beside that it should be emphasized that patients’ response and oxygenation level should be closely monitored, if insufficient it’s important to switch to invasive mechanical ventilation support without delay. Postponing intubation as much as possible and maintaining patient’s oxygenation at the required level with non-invasive approaches is mainly recommended. Although NIMV is easy to use, it increases the risk of contamination by aerosol generation. While applying NIMV, it is recommended to use a helmet or full face mask if possible and if not oronasal mask may be used. A full-face mask and oronasal mask should fit perfectly, the patient should not have a beard. NIMV is recommended to be administered with a non-vented mask by regular or dual circuit ventilators; a viral / bacterial filter should be added to the inspiratory and expiratory outputs of the circuits. If non-invasive mechanical ventilators with a single circuit are used, the filter should be placed between the exhalation port and the mask, as shown in the figure below, in non-vented
In patients not experiencing dyspnea, hypoxemia can be treated by increasing the FiO2 ratio. In these patients, O2 can be achieved at a rate of> 85% with a flow rate of 10-15 L / min by using a non-rebreather reservoir mask (bag). But during the use of a mask with reservoir, giving O2 over 60% for more than 6 hours may cause oxygen toxicity. In patients experiencing dyspnea noninvasive respiratory support systems are usually used. In conscious patients; in addition to the reservoir oxygen mask a high flow nasal cannula (High Flow Nasal Cannula-HFNC) that can supply 21-100% O2 with a flow rate of up to 60L / min, continuous positive airway pressure (CPAP) or non-invasive mechanical ventilation (NIMV) is implemented. Beside that it should be emphasized that patients’ response and oxygenation level should be closely monitored, if insufficient it’s important to switch to invasive mechanical ventilation support without delay. Postponing intubation as much as possible and maintaining patient’s oxygenation at the required level with non-invasive approaches is mainly recommended. Although NIMV is easy to use, it increases the risk of contamination by aerosol generation. While applying NIMV, it is recommended to use a helmet or full face mask if possible and if not oronasal mask may be used. A full-face mask and oronasal mask should fit perfectly, the patient should not have a beard. NIMV is recommended to be administered with a non-vented mask by regular or dual circuit ventilators; a viral / bacterial filter should be added to the inspiratory and expiratory outputs of the circuits. If non-invasive mechanical ventilators with a single circuit are used, the filter should be placed between the exhalation port and the mask, as shown in the figure below, in non-vented
masks the ones equipped with a valve should be preferred. Humidifiers should not be used during NIMV. In patients undergoing invasive mechanical ventilation prior to any procedure and caregiving sedatization is recommended to minimize the patient’s effort.
Non-vented full face mask (left)
non-vented oronasal mask (right)
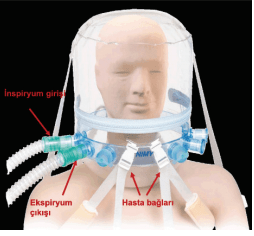
Helmet mask; There are three entrances on each side. Inspiratory line, expiratory line and a line for the passage of other apparatus such as nasogastric tube. Inputs are used according to the side position of the ventilator. Viral/bacterial filters should be installed in inspiratory and expiratory lines.
 In radiological imaging where there is a bilateral multilobar ground glass opacity that can’t be explained with pleural effusion collapse, heart failure or fluid overload and the oxygenation can’t be corrected by conventional methods the patient should be treated when possible with high-flow nasal oxygen (HFNC). Oxygen levels are regulated by increasing the oxygen flow up to maximum 60 L / min so FiO2 is maintained at <60%. The patient undergoing HFNC should wear a medical / surgical mask. Due to high flow oxygen application the risk of aerosol generation is increased so if possible patients should be treated in a negative pressure room or at least in single rooms with maximum protection with PPEs. At every stage of hypoxia the prone position can be tried for vigilant patients with lung gravity-dependent consolidation areas. Prone position is recommended at least 4 hours each time. Prone position can be considered several times a day, depending on its effect and patient tolerance. Patients who can’t tolerate the prone position should be provided to lie in the right and left lateral position. Meanwhile, the presence of tachypnea and respiratory distress should be closely monitored. Unless necessary, the connection of the mechanical ventilator circuit shouldn’t be disconnected, if it is necessary, personal protective equipment must be used. When possible, closed system suction method should be used, circuit, closed suction system and filters should not be changed routinely.
In radiological imaging where there is a bilateral multilobar ground glass opacity that can’t be explained with pleural effusion collapse, heart failure or fluid overload and the oxygenation can’t be corrected by conventional methods the patient should be treated when possible with high-flow nasal oxygen (HFNC). Oxygen levels are regulated by increasing the oxygen flow up to maximum 60 L / min so FiO2 is maintained at <60%. The patient undergoing HFNC should wear a medical / surgical mask. Due to high flow oxygen application the risk of aerosol generation is increased so if possible patients should be treated in a negative pressure room or at least in single rooms with maximum protection with PPEs. At every stage of hypoxia the prone position can be tried for vigilant patients with lung gravity-dependent consolidation areas. Prone position is recommended at least 4 hours each time. Prone position can be considered several times a day, depending on its effect and patient tolerance. Patients who can’t tolerate the prone position should be provided to lie in the right and left lateral position. Meanwhile, the presence of tachypnea and respiratory distress should be closely monitored. Unless necessary, the connection of the mechanical ventilator circuit shouldn’t be disconnected, if it is necessary, personal protective equipment must be used. When possible, closed system suction method should be used, circuit, closed suction system and filters should not be changed routinely.
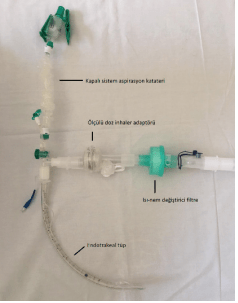
Closed system circuit assembly example; A viral/bacterial filter is placed at the inspiratory and expiratory output. Normally, the metered dose inhaler adapter or nebulizer is placed in the inspiration line, but in the presence of a heat-moisture exchanger filter, the adapter is placed in front of the filter in order to not disrupt the circuit integrity. If active humidification with heating will be applied instead of heat-moisture exchanger filter, metered dose inhaler adapter is placed in the inspiration line.
2.3. Cardiopulmonary resuscitation
According to “Adult Advanced Life Support Algorithm for COVID-19 Patients” prepared by the Resuscitation Association, chest compressions or airway procedures should not be performed before wearing full PPE due to the risk of aerosol generation and high risk of infection. The same way full PPEs should be worn during chest compressions (if non-shockable rhythm) or defibrillation (shockable rhythm). Since wearing PPEs may delay the application of Cardiopulmonary Resuscitation (CPR), it is very important to keep PPEs ready in the resuscitation cart and to recognize the deterioration in the patient’s condition at an early stage. Resuscitation should be performed with as few people as possible. If the patient is not intubated and is Bag-Valve-Mask (BVM) ventilated (face mask) the mask should not be removed from the patient’s face during chest compressions. If the patient is manually ventilated small tidal volumes should be performed. The Bag-Valve-Mask should be equipped with a viral / bacterial filter. An experienced healthcare professional should perform intubation preferably with the help of a video laryngoscope. The patient should not ventilate with Bag-Valve-Mask for a long time. The use of ETCO2 to check the intubation tube’s level should be avoided. As the risk of droplet spreading will increase during ETCO2 insertion and removal, the level of the tube should be checked by listening the lungs ventilation with a stethoscope. Open suction should be avoided before, during and after intubation. Necessary analgesia and sedative drugs should be used to ensure adequate muscle relaxation before intubation.
2.4. Delirium Assessment and Management
Delirium is defined as fluctuation of consciousness within days and hours accompanied by cognitive and perceptual disorders and attention deficit. The official definition of delirium in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) requires a disturbance in attention and awareness that develops acutely and tends to fluctuate. Delirium is characterized by an acute change in cognition (disorientation, memory loss, speech and perception disorders) and a disturbance of consciousness, usually resulting from an underlying medical problem, that develops over a short period of time (usually hours to days) and tends to fluctuate during the course of a day. A similar situation may also be valid for patients with suspected COVID-19. Delirium negatively affects the patient’s compliance with the examination and treatment process and also is accompanied by significantly higher mortality and morbidity. A day with delirium increases the length of stay in the hospital by 20% and mortality by 10%.
In COVID-19 patients delirium reasons that should be firstly considered are as follows:
- Respiratory problems, especially hypoxia.
- High fever
- Metabolic disorders
- Nutritional disorders and dehydration
- Drug side effects / interactions.
Delirium can be seen in three forms: hyperactive, hypoactive and mixed. Hypoactive delirium is manifested by decreased psychomotor function, lethargy, confusion, sedation, decreased level of consciousness and attention, withdrawal and apathy. The hyperactive delirium is accompanied by restlessness, agitation, aggression, hallucination, delusion, paranoia, disorientation and the behavior of pulling invasive instruments from the body. In order to prevent the patient and others from getting injured restrictions are applied. Restriction procedure is planned by the physician and applied by the nurse. Skin integrity and circulatory status of the restrained patient is checked by the nurse every hour. Patients place and time orientation are evaluated daily, pain control is applied and explanations about the intensive care unit and all applications should be done regularly. Sleep patterns are regulated. Environmental stimuli like sound, light, noise, etc. are reduced, active-passive Rom exercises may be performed and if possible early mobilization should be provided. Voice records from family members and pictures can be used as the part of therapy.
Resources
- https: //covid19bilgi.saglik.gov.tr/tr/covid-19-yeni-koronavirus-hastaligi-nedir.html, July 1,2020.
- Abir M, Nelson C, Chan EW, et al. Critical care surge response strategies for the 2020 COVID-19 outbreak in the United States. https://www.rand.org/content/dam/rand/pubs/research_reports/RRA100/RRA164-1/RAND_RRA164-1.pdf, July 1, 2020.
- https: //covid19.who.int/, July 1, 2020.
- World Health Organization (WHO) (2020). Health Systems Respond to COVID-19 Technical Guidance Creating surge capacity for acute and intensive care Recommendations for the WHO European Region, April 6, 2020. https://www.euro.who.int/__data/assets/pdf_file/0006/437469 /TG2-CreatingSurgeAcuteICUcapacity-eng.pdf, (6 April 2020).
- Kebapcı A. Current Approaches to Treatment and Care Interventions in Intensive Care Units of COVID-19 Patients. Journal of Intensive Care Nursing 2020; 24 (ANNEX-1): 46-56
- Acıbadem Health Group, Intensive Care Unit Covid-19 Patient Care Instruction, July 1, 2020.
- https: //covid19bilgi.saglik.gov.tr/depo/afisler/Saglik_Personeli/COVID-19_KKE_UYGUN_KULLANIMI_AFIS_A4.pdf, July 1, 2020.
- T.C. Ministry of Health, General Directorate of Public Health. (2020). COVID-19 (SARS-CoV-2 Infection Severe Pneumonia, ARDS, Sepsis and Shock Management) Guideline (01 June 2020)
- T.C. Ministry of Health General Directorate of Public Health. (2020). COVID-19 (SARSCoV-2 Infection Adult Patient Treatment) Guide (June 19, 2020) (Access Date: 02.07.2020) https://covid19bilgi.saglik.gov.tr/depo/rehberler/covid-19-rehberi/COVID- 19_REHBERI_ERISKIN_HASTA_TEDAVISI.pdf
- Gattinoni L, Chiumello D, Caironi P, Busana M, Romitti F, Brazzi L, & Camporota L. COVID-19 pneumonia: different respiratory treatments for different phenotypes ?. Intensive care medicine. 2020, 1.
- Brewster DJ, Chrimes NC, Do TB., Fraser K, Groombridge CJ, Higgs A, & Nickson CP. Consensus statement: Safe Airway Society principles of airway management and tracheal intubation specific to the COVID-19 adult patient group. Med J Aust .2020, 16.
- Resuscitation Association. (2020). Adult Advanced Life Support Algorithm for COVID-19 Patients, http://resusitation.org/tr/etkinlilikhaberler/ 291-covid-19-patients-in-medical-advanced-life-support algorithm.html, July 1, 2020.
- Özdemir L. Management of Delirium in Intensive Care Patients and Responsibilities of Nurses The Management of Delirium in Intensive Care Patients and the Responsibilities of Nurses. Hacettepe University Nursing Faculty Journal 2014, 90–98.
- With Special Notes For Covid-19 And Its Treatment: Psychiatric Assessment And Treatment In Delirium And Deficiency https://www.psikiyatri.org.tr/TPDData/Uploads/files/DeliryumYoksunlukCOVID.pdf, July 14, 2020.
- Delirium in Intensive Care. http://www.tihud.org.tr/uploads/content/kongre/5/5.13.pdf, July 14, 2020.
Prepared by: Ayça Gençoğlu Toprak
Acıbadem Healthcare Group
Training and Development Nurse
Preparation Date: 02.07.2020
Prepared by: Satı Kalkan
Acıbadem Healthcare Group
İnternational Hospital, Nursing Services Manager
Preparation Date: 02.07.2020